Each 5 mL contains Phenytoin Sodium 250 mg.
Compatible solution: 0.9% Sodium Chloride.
The solution should be clear, colorless solution without precipitation or haziness when diluted.
Pharmacology: Pharmacodynamics: Phenytoin is an anticonvulsant drug which may be useful in the treatment of epilepsy. The primary site of action appears to be the motor cortex where spread of seizure activity is inhibited. Possibly by promoting sodium efflux from neurons, phenytoin tends to stabilize the threshold against hyperexcitability caused by excessive stimulation or environmental changes capable of reducing membrane sodium gradient. This includes the reduction of post-tetanic potentiation at the synaptic levels. Loss of post-tetanic potentiation prevents cortical seizure foci from detonating adjacent cortical areas. Phenytoin reduces the maximal activity of brain stem centers responsible for the tonic phase of tonic-clonic (grand mal) seizures.
Pharmacokinetics: Phenytoin is a weak acid and has limited hydrosolubility, even in the intestine. The compound undergoes a slow and somewhat variable absorption after oral administration. After intramuscular administration, the absorption of phenytoin is slower than after oral administration, due to poor hydrosolubility of the compound and the possibility of its precipitation at the site of injection.
The plasma half-life of phenytoin in man averages 22 hours with a range of 7 to 42 hours. Phenytoin has an apparent volume of distribution of 0.6L/Kg and is highly bound (90%) plasma proteins, mainly albumin. Free phenytoin levels may be altered in patients whose protein binding characteristics differ from normal. Phenytoin is distributed into cerebrospinal fluid (CSF), saliva, semen, gastrointestinal fluids, bile, and breast milk. The concentration of phenytoin in CSF, brain, and saliva approximates the level of free phenytoin in plasma.
Phenytoin is biotransformed in the liver by oxidative metabolism. The major pathway involves 4-hydroxylation, which accounts for 80% of all metabolites. CYP2C9 plays the major role in the metabolism of phenytoin (90% of net intrinsic clearance), while CYP2C19 has a minor involvement in this process (10% of net intrinsic clearance). This relative contribution of CYP2C19 to phenytoin metabolism may however increase at higher phenytoin concentrations.
Because the cytochrome systems involved in phenytoin hydroxylation in the liver are saturable at high serum concentrations, small incremental doses of phenytoin may increase the half-life and produce very substantial increases in serum levels when these are in or above the upper therapeutic range. The clearance of phenytoin has been shown to be impaired by CYP2C9 inhibitors such as phenylbutazone and sulphaphenazole. Impaired clearance has also been shown to occur in patients administered CYP2C19 inhibitors such as ticlopidine. Most of the drug is excreted in the bile as inactive metabolites which are then reabsorbed from the intestinal tract and eliminated in the urine partly through glomerular filtration but, more importantly via tubular secretion. Less than 5% of phenytoin is excreted as the parent compound.
A fall in phenytoin serum levels may occur when patients are switched from oral to intramuscular (IM) administration. The drop is caused by slower absorption, as compared to oral administration, due to the poor hydrosolubility of phenytoin and the possibility of its precipitation at the site of injection. Intravenous administration is the preferred route for producing rapid therapeutic serum levels.
Phenytoin Sodium Injection is indicated for the control of status epilepticus of the tonic-clonic (grand mal) type and prevention and treatment of seizures occurring during or following neurosurgery.
General: Phenytoin capsules and solution for injection are formulated with the sodium salt of phenytoin. The free acid form of phenytoin is used in the phenytoin suspension (30mg/5mL (paediatric) and 125mg/5mL) and in the phenytoin tablets. Because there is approximately an 8% increase in drug content with the free acid form over that of the sodium salt, dosage adjustments and serum level monitoring may be necessary when switching from a product formulated with the free acid to a product formulated with the sodium salt and vice versa.
Phenytoin serum level determinations may be necessary to achieve optimal dosage adjustments.
Optimum control without clinical sign of toxicity occurs most often with serum levels between 10 and 20mcg/ml.
Parenteral Phenytoin may be administered as a slow intravenous (IV) bolus or it may be administered via an IV infusion.
Because of the risk of local toxicity, intravenous phenytoin should be administered directly into a large peripheral or central vein through a large-gauge catheter. Prior to the administration, the patency of the IV catheter should be tested with a flush of sterile saline. Each injection or infusion of parenteral phenytoin should then be preceded and followed by a flush of sterile saline through the same needle or catheter to avoid local venous irritation due to the alkalinity of the solution.
Local Toxicity including (Purple Glove Syndrome): Bolus Administration: A bolus of Phenytoin Sodium Injection should be injected slowly, not exceeding 50mg per minute in adults, into a large vein through a large-gauge needle or intravenous catheter. Each injection of intravenous phenytoin should be preceded by a saline flush and followed by an injection of sterile saline through the same needle or catheter to avoid local venous irritation due to the alkalinity of the solution.
Infusion Administration: For administration by infusion, Phenytoin Sodium Injection should be diluted in 50-100ml of normal saline with the final concentration of phenytoin in the solution not exceeding 10mg/ml. Administration should commence immediately after the mixture has been prepared and must be completed within one hour (the infusion mixture should not be refrigerated). An in-line filter (0.22-0.50 microns) should be used. Each injection of intravenous phenytoin should be preceded by a saline flush and followed by an injection of sterile saline through the same needle or intravenous catheter to help reduce local venous irritation due to the alkalinity of the solution.
Dosage is not to exceed 50 mg/minute, intravenously in adults, and not to exceed 1-3 mg/kg/minute in neonates and children. There is a relatively small margin between full therapeutic effect and minimally toxic doses of this drug.
On those occasions when intramuscular administration may be required (i.e., postoperatively in comatose patients), a sufficient dose must be administered intramuscularly to maintain the serum level within the therapeutic range. Where oral dosage is resumed following IM usage, the oral dosage should be adjusted to compensate for the slow, continuing IM absorption to avoid toxic symptoms. To avoid drug accumulation due to absorption from the muscle depots, it is recommended that for the first week back on oral phenytoin, the oral dose be reduced to one-half of the original dose (one-third of the IM dose).
Status Epilepticus: In adults a loading dose of 10 to 15 mg/kg should be administered slowly intravenously, at a rate not exceeding 50 mg per minute (this will require approximately 20 minutes in a 70 kg patient). The loading dose should be followed by a maintenance dose of 100 mg orally or intravenously every 6 to 8 hours.
Absorption of phenytoin in neonates and children may be unreliable after oral administration. A loading dose of 15-20mg/kg of phenytoin intravenously will usually produce serum concentrations of phenytoin within the generally accepted therapeutic range (10-20 mcg/mL). The drug should be injected slowly intravenously at a rate not exceeding 1-3 mg/kg/minute.
Continuous monitoring of the electrocardiogram and blood pressure is essential. The patient should be observed for signs of respiratory depression. Determination of phenytoin serum levels is advised when using phenytoin in the management of status epilepticus and in the subsequent establishment of maintenance dosage.
Other measures including concomitant administration of an intravenous benzodiazepine such as diazepam, or intravenous short-acting barbiturate, will usually be necessary for rapid control of seizures because of the required slow rate of administration of phenytoin. If administration of parenteral phenytoin does not terminate seizures, the use of other anticonvulsants, intravenous barbiturates, general anesthesia, or other appropriate measures should be considered.
Intramuscular administration should not be used in the treatment of status epilepticus because the attainment of peak serum levels may require up to 24 hours.
Neurosurgery: Prophylactic dosage - 100 to 200 mg (2 to 4 mL) intramuscularly at approximately 4 hour intervals during surgery and continued during the postoperative period. When intramuscular administration is required for a patient previously stabilized orally, compensating dosage adjustments are necessary to maintain therapeutic serum levels. When intramuscular administration is used, the drug should be given by deep intramuscular injection. An intramuscular dose 50% greater than the oral dose is necessary to maintain these levels. When the patient is returned to oral administration, the dose should be reduced by 50% of the original oral dose for one week to prevent excessive serum levels due to sustained release form intramuscular tissue sites.
If the patient requires more than one week of IM phenytoin, alternative routes should be explored, such as gastric intubation. For time periods less than one week, the patient shifted back from IM administration should receive one-half the original oral dose for the same period of time the patient received IM phenytoin. Monitoring serum levels would help prevent a fall into the subtherapeutic range. Serum drug level determinations are especially helpful when possible drug interactions are suspected.
Route of Administration: Parenteral.
[Intramuscular, Intravenous.]
The lethal dose in pediatric patients is not known. The lethal dose in adults is estimated to be 2 to 5 grams. The initial symptoms are nystagmus, ataxia, and dysarthria. Other signs are tremor, hyperreflexia, somnolence, drowsiness, lethargy, slurred speech, blurred vision, nausea, vomiting. The patient may become comatose and hypotensive. Death is due to respiratory and circulatory depression. There are marked variations among individuals with respect to phenytoin serum levels where toxicity may occur. Nystagmus on lateral gaze usually appears at 20mcg/mL and ataxia at 30mcg/mL, dysarthria and lethargy appear when the serum concentration is >40mcg/mL, but a concentration as high as 50mcg/mL has been reported without evidence of toxicity. As much as 25 times the therapeutic dose has been taken to result in a serum concentration >100mcg/mL with complete recovery.
Treatment: Treatment is non-specific since there is no known antidote. The adequacy of the respiratory and circulatory systems should be carefully observed and appropriate supportive measures employed. Hemodialysis can be considered since phenytoin is not completely bound to plasma proteins. Total exchange transfusion has been in the treatment of severe intoxication in pediatric patients.
In acute overdosage the possibility of the presence of other CNS depressants, including alcohol, should be in mind.
Phenytoin is contraindicated in those patients who are hypersensitive to phenytoin, or its inactive ingredients, or other hydantoins. Because of its effect on ventricular automaticity, phenytoin is contraindicated in sinus bradycardia, sino-atrial block, second and third degree A-V block, and in patients with Adams-Stokes syndrome.
Co-administration of phenytoin is contraindicated with delavirdine due to the potential for loss of virologic response and possible resistance to delavirdine or to the class of non-nucleoside reverse transcriptase inhibitors.
Phenytoin is not effective for absence (petit mal) seizures. If tonic-clonic (grand mal) and absence (petit mal) seizures are present, combined drug therapy is needed.
Phenytoin is not indicated for seizures due to hypoglycemia or other metabolic causes.
Appropriate diagnostic procedures should be performed as indicated.
The most significant signs of toxicity with the intravenous use of phenytoin are cardiovascular collapse and/or central nervous system depression. Hypotension does occur when the drug is administered rapidly by the intravenous route. The rate of administration is very important; it should not exceed 50 mg per minute in adults, and 1-3 mg/kg/minute in neonates and children.
At this rate, toxicity should be minimized.
Hypotension usually occurs when the drug is administered by the intravenous route.
Phenytoin should be used with caution in patients with hypotension and severe myocardial insufficiency.
The intramuscular route is not recommended for the treatment of status epilepticus since serum levels of phenytoin in the therapeutic range cannot be readily achieved with doses and methods of administration ordinarily used. In the treatment of status epilepticus, the intravenous route is preferred because of the delay in absorption of phenytoin when administered intramuscularly.
Antiepileptic drugs should not be abruptly discontinued because of the possibility of increased seizure frequency, including status epilepticus. When, in the judgment of the clinician, the need for dosage reduction, discontinuation, or substitution of alternative antiepileptic medication arises, this should be done gradually. However, in the event of an allergic or hypersensitivity reaction, rapid substitution of alternative therapy may be necessary. In this case, alternative therapy should be an antiepileptic drug not belonging to the hydantoin chemical class.
A small percentage of individuals who have been treated with phenytoin have been shown to metabolize the drug slowly. Slow metabolism may be due to limited enzyme availability and lack of induction; it appears to be genetically determined (polymorphism).
Acute alcoholic intake may increase phenytoin serum levels while chronic alcoholic use may decrease serum levels.
Several individual case reports have suggested that there may be an increased, although still rare, incidence of hypersensitivity reactions, including skin rash and hepatotoxicity, in black patients.
Suicide: Suicidal ideation and behaviour have been reported in patients treated with antiepileptic agents in several indications. A meta-analysis of randomised placebo-controlled trials of anti-epileptic drugs has also shown a small increased risk of suicidal ideation and behaviour. The mechanism of this risk is not known and the available data do not exclude the possibility of an increased risk for Phenytoin.
Potential for an increase in risk of suicidal thoughts or behaviors.
Cardiovascular Effect: Severe cardiotoxic reactions and fatalities have been reported with atrial and ventricular depression and ventricular fibrillation.
Severe complications are most commonly encountered in elderly or gravely ill patients.
Local Toxicity (including Purple Glove Syndrome): Soft tissue irritation and inflammation have occurred at the site of injection with and without extravasation of intravenous phenytoin.
Edema, discoloration and pain distal to the site of injection (described as "purple glove syndrome") have been reported following peripheral intravenous phenytoin injection. Soft tissue irritation may vary from slight tenderness to extensive necrosis, and sloughing of skin. The syndrome may not develop for several days after injection. Although resolution of symptoms may be spontaneous, skin necrosis and limb ischemia have occurred and required such interventions as fasciotomies, skin grafting, and, in rare cases, amputation.
Improper administration including subcutaneous or perivascular injection should be avoided.
Intramuscular phenytoin administration may cause pain, necrosis, and abscess formation at the injection site.
Hypersensitivity Syndrome/ Drug Reaction with Eosinophilia and Systemic Symptoms (HSS/DRESS): Hypersensitivity Syndrome (HSS) or Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) has been reported in patients taking anticonvulsant drugs, including phenytoin. Some of these events have been fatal or life threatening.
HSS/DRESS typically, although not exclusively, presents with fever, rash, and/or lymphadenopathy, in association with other organ system involvement, such as hepatitis, nephritis, hematological abnormalities, myocarditis, myositis or pneumonitis. Initial symptoms may resemble an acute viral infection. Other common manifestations include arthralgias, jaundice, hepatomegaly, leukocytosis, and eosinophilia. The interval between first drug exposure and symptoms is usually 2-4 weeks, but has been reported in individuals receiving anticonvulsants for 3 or more months. If such signs and symptoms occur, the patient should be evaluated immediately. Phenytoin should be discontinued if an alternative aetiology for the signs and symptoms cannot be established.
Patients at higher risk for developing HSS/DRESS include black patients, patients who have experienced this syndrome in the past, (with phenytoin or other anticonvulsant drugs), patients who have a family history of this syndrome and immune-suppressed patients.
The syndrome is more severe in previously sensitized individuals.
Serious Dermatologic Reactions: Phenytoin can cause rare, serious skin adverse events such as exfoliative dermatitis, Stevens-Johnson Syndrom (SJS), and toxic epidermal necrolysis (TEN), which can be fatal. Although serious skin reactions may occur without warning, patients should be alert for the occurrence of rash and other symptoms of HSS/DRESS and should seek medical advice from their physician immediately when observing any indicative signs or symptoms. The physician should advise the patient to discontinue treatment if the rash appears. If the rash is of a milder type (measles-like or scarlantiniform), therapy may be resumed after the rash has completely disappeared. If the rash recurs upon reinstitution of therapy, further phenytoin medication is contraindicated. The risk of serious skin reactions and other hypersensitivity reactions to phenytoin may be higher in black patients.
Hepatic Injury: The liver is the chief site of biotransformation of phenytoin. Toxic hepatitis and liver damage have been reported and may, in rare cases, be fatal.
Cases of acute hepatotoxicity, including infrequent cases of acute hepatic failure, have been reported with phenytoin. These incidents usually occur within the first 2 months of treatment and may be associated with HSS/DRESS. Patients with impaired liver function, elderly patients, or those who are gravely ill may show early signs of toxicity.
The clinical course of acute phenytoin hepatotoxicity ranges from prompt recovery to fatal outcomes. In these patients with acute hepatotoxicity, phenytoin should be immediately discontinued and not re-administered.
The risk of hepatotoxicity and other hypersensitivity reactions to phenytoin may be higher in black patients.
Hematopoietic System: Hematopoietic complications, some fatal, have occasionally been reported in association with administration of phenytoin. These have included thrombocytopenia, leukopenia, granulocytopenia, agranulocytosis, and pancytopenia with or without bone marrow suppression.
There have been a number of reports suggesting a relationship between phenytoin and the development of lymphadenopathy (local or generalized) including benign lymph node hyperplasia, pseudolymphoma, lymphoma, and Hodgkin's disease. Although a cause and effect relationship has not been established, the occurrence of lymphadenopathy indicates the need to differentiate such a condition from other types of lymph node pathology. Lymph node involvement may occur with or without symptoms and signs resembling HSS/DRESS. In all cases of lymphadenopathy, follow-up observation for an extended period is indicated and every effort should be made to achieve seizure control using alternative anticonvulsant drugs.
While macrocytosis and megaloblastic anemia have occurred, these conditions usually respond to folic acid therapy. If folic acid is added to phenytoin therapy, a decrease in seizure control may occur.
Central Nervous System Effect: Serum levels of phenytoin sustained above the optimal range may produce confusional states referred to as "delirium", "psychosis", or "encephalopathy", or rarely irreversible cerebellar dysfunction. Accordingly, at the first sign of acute toxicity, serum drug level determinations are recommended. Dose reduction of phenytoin therapy is indicated if serum levels are excessive; if symptoms persist, termination of therapy with phenytoin is recommended.
Metabolic Effect: In view of isolated reports associating phenytoin with exacerbation of porphyria, caution should be exercised in using this medication in patients suffering from this disease. Hyperglycemia, resulting from the drug's inhibitory effects on insulin release, has been reported. Phenytoin also may raise serum glucose levels in diabetic patients.
Information for the Patient: Patients should be cautioned on the use of other drugs or alcoholic beverages without first seeking their physician's advice.
Patients should be instructed to call their physician if skin rash develops.
Effects on Ability to Drive and Use Machine: Patients should be advised not to drive a car or operate potentially dangerous machinery until it is known that this medication does not affect their ability to engage in these activities.
Pregnancy: A number of reports suggest an association between the use of anticonvulsant drugs by women with epilepsy and a higher incidence of birth defects in children born to these women. Data are more extensive with respect to phenytoin and phenobarbital, but these are also the most commonly prescribed anticonvulsant drugs.
The reports suggesting a higher incidence of birth defects in children of drug-treated epileptic women cannot be regarded as adequate to prove a definite cause and effect relationship. There are intrinsic methodologic problems in obtaining adequate data on drug teratogenicity in humans. Genetic factors or the epileptic condition itself may be more important than drug therapy in leading to birth defects. The great majority of mothers on anticonvulsant medication deliver normal infants. It is important to note that anticonvulsant drugs should not be discontinued by patients in whom the drugs is administered to prevent major seizures because of the strong possibility of precipitating status epilepticus with attendant hypoxia and threat to life. In individual cases where the severity and frequency of the seizure disorder are such that the removal of medication does not pose a serious threat to the patient, discontinuation of the drug may be considered prior to and during pregnancy although it cannot be said with any confidence that even minor seizures do not pose some hazard to the developing embryo or fetus. The prescribing physician will wish to weigh these consideration in treating or counselling epileptic women of child-bearing potential.
In addition to the reports of increased incidence of congenital malformations such as cleft lip/palate and heart malformations in children of women who received phenytoin and other anticonvulsant drugs, there have been reports of a fetal hydantoin syndrome. This consists of prenatal growth deficiency, microcephaly, and mental deficiency in children born to mothers who have received phenytoin, alcohol, barbiturates or trimethadione. However, these features are all interrelated and are frequently associated with intrauterine growth retardation from other causes.
There have been isolated reports of malignancies, including neuroblastoma, in children whose mothers received phenytoin during pregnancy.
An increase in seizure frequency during pregnancy occurs in a proportion of patients, because of altered phenytoin absorption or metabolism. Periodic measurement of serum phenytoin levels is particularly valuable in the management of a pregnant epileptic patient as a guide to an appropriate adjustment of dosage. However, postpartum restoration of the original dosage will probably be indicated. Neonatal coagulation defects have been reported within the first 24 hours in babies born to epileptic mothers receiving phenobarbital and/or phenytoin. Vitamin K has been shown to prevent or correct this defect and has been recommended to be given to the mother before delivery and to the neonate after birth.
Lactation: Infant breast-feeding is not recommended for women taking this drug because phenytoin appears to be secreted in low concentrations in human milk. Phenytoin concentration in breast milk is approximately one-third of the corresponding maternal plasma concentration.
The following adverse reactions have been reported with phenytoin.
Body as a Whole: Anaphylactoid reaction, and anaphylaxis.
Cardiovascular System: Hypotension has been observed.
Central Nervous System: Adverse reactions in this body system are common and are usually dose-related. Reactions include nystagmus, ataxia, slurred speech, decreased coordination, and mental confusion.
Dizziness, vertigo, insomnia, transient nervousness, motor twitching, headache, parasthesia and somnolence have also been observed. There have also been reports of phenytoin-induced dyskinesia, including chorea, dystonia, tremor, and asterixis, similar to those induced by phenothiazine and other neuroleptic drugs.
A predominantly sensory peripheral polyneuropathy has been observed in patients receiving long-term phenytoin therapy.
Connective Tissue System: Coarsening of the facial features, enlargement of the lips, gingival hyperplasia, hypertrichosis, and Peyronie's disease.
Gastrointestinal System: Acute hepatic failure, toxic hepatitis, liver damage, vomiting, nausea, constipation.
Hematopoietic System: Hematopoietic complications, some fatal, have occasionally been reported in association with administration of phenytoin. These have included thrombocytopenia, leukopenia, granulocytopenia, agranulocytosis, and pancytopenia with or without bone marrow suppression. Macrocytosis and megaloblastic anemia have also occurred. Lymphadenopathy including benign lymph node hyperplasia, pseudolymphoma, lymphoma, and Hodgkin's disease have been reported.
Immunologic: Hypersensitivity syndrome/Drug reaction with eosinophilia and systemic symptoms (HSS/DRESS), systemic lupus erythematosus, periarteritis nodosa, and immunoglobulin abnormalities.
Injection Site: Local irritation, inflammation, tenderness, necrosis, and sloughing of skin have been reported with or without extravasation of intravenous phenytoin. Edema, discolouration and pain distal to the site of injection (described as "purple glove syndrome") have also been reported.
Dermatologic System: Dermatological manifestations, sometimes accompanied by fever, have included scarlatiniform or morbiliform rashes. A morbiliform rash (measles-like) is the most common; other types of dermatitis are seen more rarely. Other more serious forms which may be fatal have included bullous, exfoliative, or purpuric dermatitis, lupus erythematosus, Steven-Johnson syndrome, and toxic epidermal necrolysis.
Special Senses: Taste perversion.
Drug Interactions: Phenytoin is extensively bound to serum plasma proteins and is prone to competitive displacement. Phenytoin is metabolized by hepatic cytochrome (CYP) P450 enzymes CYP2C9 and CYP2C19 and is particularly susceptible to inhibitory drug interactions because it is subject to saturable metabolism. Inhibition of metabolism may produce significant increases in circulating phenytoin concentrations and enhance the risk of drug toxicity.
Phenytoin is a potent inducer of hepatic drug metabolizing enzymes and may reduce the levels of drugs metabolized by these enzymes.
There are many drugs which may increase or decrease serum phenytoin levels or which phenytoin may affect. Serum level determinations for phenytoin are especially helpful when possible drug interactions are suspected.
The most commonly occurring drug interactions are listed as follows.
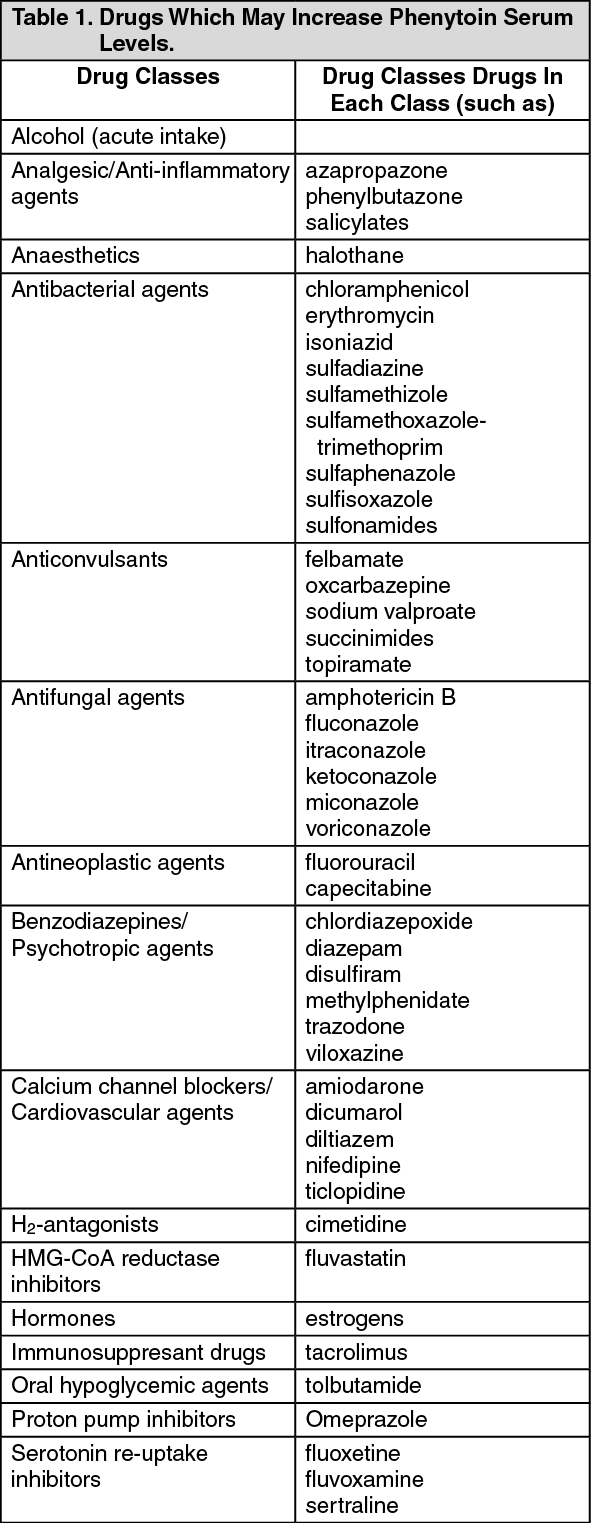
Drugs which may increase phenytoin serum levels: Table 1 summarizes the drug classes which may potentially increase phenytoin serum levels. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
This list is not intended to be inclusive or comprehensive. Individual drug labels should be consulted.
Drugs which may decrease phenytoin serum levels: Table 2 summarizes the drug classes which may potentially decrease phenytoin serum levels. (See Table 2.)
Click on icon to see table/diagram/image
This list is not intended to be inclusive or comprehensive. Individual drug labels should be consulted.
Molindone hydrochloride contains calcium ions which interfere with the absorption of phenytoin. Ingestion times of phenytoin and calcium preparations, including antacid preparations containing calcium, should be staggered to prevent absorption problems.
Drugs which may increase or decrease phenytoin serum levels: Table 3 summarizes the drug classes which may either increase or decrease phenytoin serum levels. (See Table 3.)
Click on icon to see table/diagram/image
This list is not intended to be inclusive or comprehensive. Individual drug labels should be consulted.
Drugs whose serum levels and/or effects may be altered by phenytoin: Table 4 summarizes the drug classes whose serum levels and/or effects may be altered by phenytoin. (See Table 4.)
Click on icon to see table/diagram/image
This list is not intended to be inclusive or comprehensive. Individual drug labels should be consulted.
Although not a true drug interaction, tricyclic antidepressants may precipitate seizures in susceptible patients and phenytoin dosage may need to be adjusted.
Drug-Enteral Feeding / Nutrition Preparations Interaction: Literature reports suggest that patients who have received enteral feeding preparations and/or related nutritional supplements have lower than expected phenytoin plasma levels. It is therefore suggested that phenytoin not be administered concomitantly with an enteral feeding preparation.
More frequent serum phenytoin level monitoring may be necessary in these patients.
Drug/Laboratory Test Interactions: Phenytoin may cause decreased serum levels of protein-bound iodine (PBI). It also may produce lower than normal values for dexamethasone or metyrapone tests. Phenytoin may cause increased serum levels of glucose, alkaline phosphatase, and gamma glutamyl-transpeptidase (GGT). Phenytoin may affect blood calcium and blood sugar metabolism tests.
Incompatibilities: The mixing of phenytoin sodium injection with other drugs is not recommended because of precipitation of phenytoin acid.
After dilution: Administration should commence immediately after the mixture has been prepared and must be completed within one hour (the infusion mixture should not be refrigerated).
Store below 30°C.
Do not freeze.
Protect from light.
Shelf-Life: 36 months.
N03AB02 - phenytoin ; Belongs to the class of hydantoin derivatives antiepileptics.
Pharmaniaga Phenytoin Na inj 250 mg/5 mL
10 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image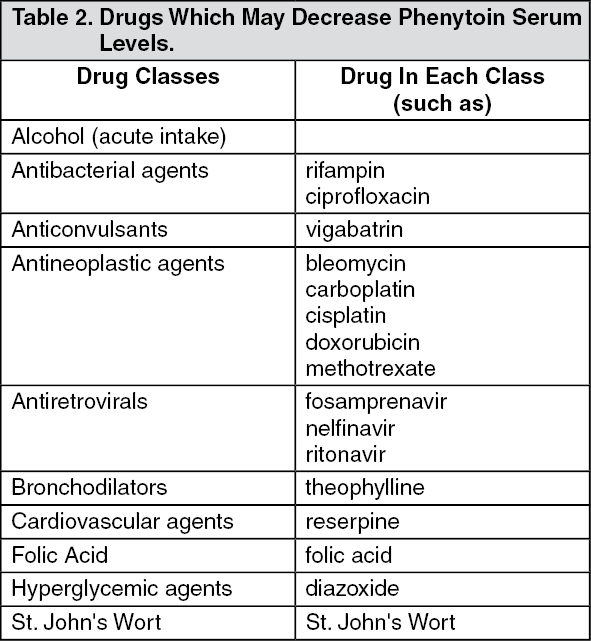 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
